Health and social change in Latvia 1991–2001 – a modern piece of medical history
Michael 2004; 1: 277–85.
Health and social changes in Latvia
Latvia, the small country at the Baltic Sea had been part of the Soviet Union since 1940, but regained its status as an independent state in 1991. At this point, health and social conditions resembled those in other former Soviet states in the Western parts of the Union, and the infrastructure of the society, including the health care system was Soviet style.
Latvia has a population of 2.42 million, and around half of them live in the capital of Riga. The ethnic composition in the country is 56.5 % Latvians, 30.4 % Russians and 13.1 % others. Life expectancy is 73.7 years for women, 61.2 years for men. Gross domestic product per capita in the year 2000 was USD 2420.
For a comparison, another Nordic country, Norway, has a population of 4.50 million which is composed of 94.1 % Norwegians and 5.9 % immigrants of different origins. Life expectancy is 81.1 years for women and 75.6 % for men. Gross domestic product per capita (2000) was USD 35004, of which 8.0 % were total expenditures on health.
Since 1991 the Latvian society has undergone profound social changes, partly because of its political objective to join the European Union, where changes were required in order to qualify for application. By 2002, many traits of the Latvian society were much like in any Western European country. To achieve this goal and the further progress which is to be expected, the country has passed through a development which has been to the benefit of many groups of the population. But it has created problems in social conditions and health for others, e.g. pensioners and elderly people, or people employed in industries which were closed down due to the new market situation. The replacement of the Soviet system with a Western system in many parts of daily life, at least for a while left parts of the population in a sort of limbo which led to social difficulties and even could harm their health.
The curative part of the Soviet style health care system was mainly hospital and specialist oriented with no functioning primary health care system as such. District internists and district pediatricians were placed in policlinics together with specialists and were responsible for preventive work. After 1991 and under new financial skies, this system among other weaknesses showed to lack the required cost-effectiveness, even if e.g. its preventive potentials were quite good. The first Western style general practitioners were trained in 1992, but the political decision that a primary health care served by general practitioners should be the first line system of choice, was taken only in 1996. The process of replacing the first line specialists with trained general practitioners is long and cumbersome, and is accompanied by a process of restructuring the payment procedures for medical services.
Aims of the study
During the decade starting in 1991, the social catch-up with the Western neighbours has been so rapid, that processes lasting for many years in other countries here could be studied in compressed version. So there were two distinctive objectives: In the first place to monitor and interpret what really was going on, and in the second place to discuss the present situation in relation to the social and medical history of other countries.
Material and methods
Since 1993 the authors have had the opportunity to observe the process going on in Latvia rather closely, one of us (GK) as an internist in a Riga hospital with out-patient services, later as a general practitioner in Central Riga, the second of us (ØL) teaching medical history and community medicine at the University of Oslo with special responsibility for student outplacement in Latvia and USA, and the third (EOR) as a student tutor.
In the years 1995 to 2001 a total of 93 medical students from Oslo in groups of 4–6 twice a year stayed four weeks in Latvia as part of their training in general practice and community medicine. In the period 1996–2001 38 students had corresponding stays in the United States of America (La Crosse, Wisconsin).
Each group got to examine a given topic related to health and social change and had to write a report on their findings. They were instructed to collect as much of relevant statistical information as possible, and to supplement this with own observations and with interviews of informants and key persons in the field. In order to take care of the comparative perspective in time and space, the reports were written when the students came back to Norway and could collaborate in an evaluation of the prevalent conditions in Latvia and Norway, respectively Latvia, Norway and the United States.
However, as the reports were completed in the course of six years, the information given there is not updated beyond the year they were submitted. The outplacements were discontinued in 2001.
To provide a common background for their studies, all students took part in a standardized teaching programme in Latvia, set up by GK, presenting them to a wide series of public health issues.
The material gathered in the reports (1–12) under the guidance of the authors makes up a material fit for elucidating a piece of modern medical history – the changes in social conditions and health in Latvia.
Results – some medical and social indicators
A change in culture
In the first years following the Latvian independence, the society basically was a Soviet society, yet challenged by strong nationalistic forces urging for change. This dichotomy led to a puzzling cultural situation, as the rapid breakup from the old system on the one hand could be painful in daily life, whilst on the other hand the introduction of a Western lifestyle also could be painful, especially when resources were scarce (1). This ambiguity of course influenced the attitudes of the informants, and e.g. their evaluation of the past and their prospects for the future have to be interpreted in light of the social context:
Wrote a group who had a Latvian family as their informants in 1996 (2):
«This family lives on the eight floor in a suburb apartment building, built in the Soviet period. They have a small apartment (50 square meters) and a veranda where they dry their laundry even at minus 10 degrees Celsius. Some of the windows have synthetic curtains, and everywhere are the green plants looking more healthy than the people living there. Beneath the concrete you can easily see the rusty reinforcement. One of their children, Janis is looking at television. The Dynasty is on channel one. Krystle speaks Latvian and the subtext is in Russian. The rooms are small and the interior is dark, and Christmas decorations are everywhere even though this is late January. Migra, the grandmother, is sitting on the coach knitting mittens for sale at the market next Saturday. Unfortunately, the Latvian Cabinet recently approved new charges on electricity and hot water. However, needy elderly people like Migra have the right to receive free firewood if necessary. The pipe system is old and makes a lot of noise when the water is turned on. Often the pressure is so low that there is no water at all. The family boils their drinking water as they are recommended to do because of the spreading hepatitis A, but fruits and vegetables are eaten without washing them in advance. Chlorine is added to the drinking water, in order to prevent transmittable diseases. …»
On Ilze (i.e. the housewife and breadwinner of the family, having broken up with her husband, who is suffering from cancer of the bones following having been sent to Tsjernobyl as a cleaning up worker at the 1986 catastrophe), after describing all her worries:
«One might wonder how she is able to stand on her feet. Virtually she has no spare time, teaching and housework takes all her time. She is very pleased with her job (as a teacher), even though it is poorly paid. To us it seems peculiar that she has not developed «fibromyalgia». We tried to ask physicians about psychosomatic diseases, and they raised their eyebrows and shook their heads. They seemed to have no interest in this matter. Or could it be that patients do not complain about such problems?»
The experiences from the field work clearly show that not only the social conditions and the health priorities change rapidly, but also the attitudes towards the problems.
As can be seen from the reference list, the reports take up a series of medical topics, each of them serving as an indicator or a proxy pointing at the running medical and social processes. Important problem fields as diabetes (3), asthma (7), arterial hypertension (8), hormone replacement therapy (9) and sexually transmitted diseases (12) also were among the topics studied. Here, some examples are taken out for further presentation and discussion.
Vaccination – the rise and fall of preventive medicine?
An overview and evaluation of the vaccination programmes in the three countries was given in the report «Vaccination of children in Norway, Latvia and the United States» (6). The programmes were compared to the guidelines given by the World Health Organisation. All countries were found to have adequate vaccination schedules that were in line with their respective disease panoramas. There was, however, a need to improve the coverage level.
In the case of Latvia, coverage had been fairly good in the Soviet period, not least due to the authoritarian system. However, the new democracy had as a side effect that people did not feel as obedient and responsible as before, also when it came to following vaccination programmes.
From the Soviet time it existed a long list of contraindications, mostly due to low quality vaccines. Besides that, a diphtheria epidemic in 1994 showed that the vaccination status had not been satisfactory. Because of the new situation, supplies of vaccines to cope with the situation were not sufficient. Using new vaccines, the list of contraindications should be reduced, although new contraindications emerge, such as allergy, which in general is an increasing problem connected to the increase in living standards. Increased efforts should also be made to localize all those in need of immunization.
However, the new health care system of Latvia does not seem to support or promote vaccination as a preventive measure. As the responsibility for establishing the required degree of coverage is not clear, people have problems to respond adequately to the system changes in this field.
Tuberculosis – a proxy when studying social development
After 1990, Latvia experienced an increasing incidence of tuberculosis (4). This coincides with economic problems, such as can be shown by the inflation rates, which at the outset were around 900 per cent a year, but soon stabilized on a three percent level. However, multi-resistant strains of tuberculosis bacilli have been a special problem in Latvia, and so have the health care systems for tuberculous patients, where the staff in the hospitals are particularly exposed to be infected.
In 1995 the directly observed treatment, short course therapy (DOTS) was introduced, but Latvia has no legislation that forces patients to be treated.
Availability of antimicrobial drugs as part of freedom
In Soviet times, antibiotics and other drugs against infections were not covered by the strong regulation of drug dispensing, because they were not regarded as harmful. The use of them was in principle following the advice given by a doctor. However, the use was rather widespread, not least because antimicrobial drugs also were recommended against viral infections, such as common colds.
After 1991, this practice continued and antibiotics and related drugs could be bought over the counter without any regulations at all. At the same time there were no guidelines for the perusal, and e.g. expensive broad spectre antibiotics could be bought at the choice of the patient for minor diseases.
The students studied antibiotic practice in upper respiratory tract diseases in 1997, especially worrying about the risk of developing drug resistance in the population (5). Although Latvia seemed to pursue the same scientific objectives on use of antibacterial drugs as e.g. in Norway and the USA, i.e. a restrictive policy, the free trade in the dispensaries caused a problem, especially when economy became better: More money was available for buying expensive and fancy drugs, which might have a special harmful potential.
In 2001 prescription of antimicrobial drugs by a doctor was introduced again in Latvia.
Depression suppressed?
Depression as a primary health care problem in Latvia and Norway was discussed in a report in 2000 (11). The students found only a limited amount of literature about depression in Latvia, and there seemed to be less concern about mental health issues in Latvia as compared to Norway.
Unlike in Norway, there were no guidelines for diagnosing and treatment of depression in primary health care in Latvia.
Latvia maintains till this day a full-name register of psychiatric patients treated by specialists. A concern about patients’ anonymity was expressed. Being entered into the register may have unpleasant consequences, e.g. by application for a driver’s license. This may lead to a certain under-representation of psychiatric diagnoses. The register is by many regarded as a reminiscence of the totalitarian state.
On the other hand, there is another factor which might be of importance: In Soviet times it was a virtue to conceal one’s feelings and mental distresses. This is obviously going to change, and illnesses like depression are more likely to come to surface.
Dyspepsia as a social indicator
The report «Dyspepsia. The present status» aimed to study dyspepsia as a health problem in Latvia as compared to Norway and the USA (10). This included definition and diagnostic criteria, treatment, and distribution of risk factors, where obvious differences were to be found. Alcohol, smoking, and helicobacter pylori infection seemed to have a greater impact as risk factors in Latvia than in Norway and the USA. Relatively low prices on alcoholic beverages, and traditions for heavy drinking of strong liquor were regarded as a risk factors at hand, and so were prices, availability and habits when it came to tobacco.
Due to low cost, endoscopies were frequently performed early in the investigative process in Latvia, whilst HP-serology and urea breath test were more widely used in the other countries studied.
From a viewpoint of community medicine, the risk factors for dyspepsia deserve a closer study: Even if the old risk factors are getting less importance because of changes in habits, psychosomatic dyspepsia probably would be likely to increase. As a social indicator, dyspepsia thus points in at least two directions.
The report also focused on the research problems arising from a lack of a universal definition of dyspepsia, which among other consequences preclude more precise comparative studies.
General discussion – lessons to be learnt
The material which has been collected and interpreted, covering Latvia in the years 1993–2001, reflects a development where the country left the totalitarian order of the Soviet time, rapidly approaching standards and life style corresponding with what could be expected from a country applying for membership in the European Union.
In the field of health care, this has led to a change from a specialist and hospital oriented care to general practitioner based family medicine first line services. More and more medical guidelines are adopted guiding daily medical work, in line with in Western medicine. Increased interest in health topics may be noted in the population, but also a shift towards medical problems which were not so apparent before, partly because they belong to another stage in the development of a society, but also for reasons having to do with biology, e.g. allergy. The reports were written during a series of years when the development was going on, and the sliding of problems. solutions and attitudes can clearly be noted.
However, what has been monitored and discussed during the period covered, has to be seen as part of a larger pattern: The previous balance between personal autonomy and regulations from the authorities has been shifted, but in health matters there obviously is a need not to avoid all sorts of authoritative control and it is not possible to rely entirely on personal freedom and integrity. A new balance has to be established. The authors claim that their experiences may have bearings in time and space also for other societies undergoing changes.
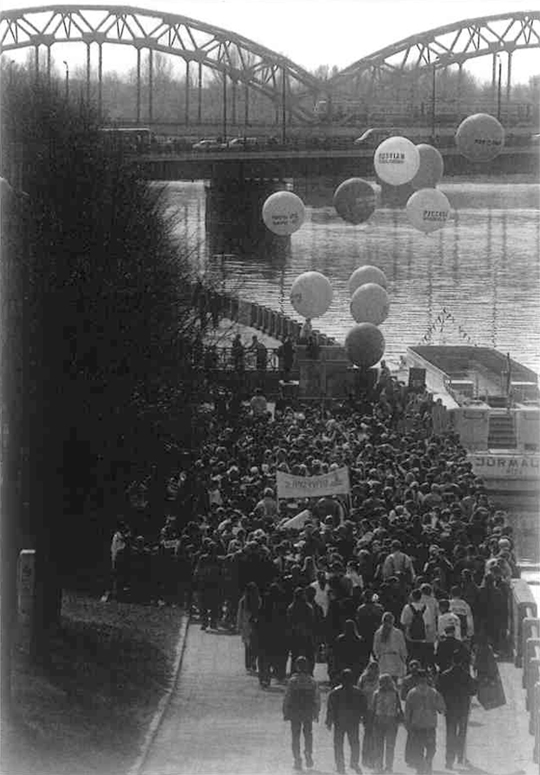
May 1, 2004 was an important day for the three Baltic countries Estonia, Latvia and Lithuania: joining the European Union. However, the minds of the people were not unanimous. An example: At the same time as celebrations were going on all over old Riga in Latvia, ethnic Russians passed the embankment of the river Daugava on their way to a demonstration to support schooling in Russian language. (Photo Ø. Larsen 2004)
References
Ancher–Olsen E, Haug LS, Hognestad A, Larsen ASF. Latvia fra et sosialistisk til et kapitalistisk helsevesen – primærhelsetjenesten i en overgangsfase. Student report, Institute of General Practice and Community Medicine, University of Oslo, Norway, 1995.
Fryjordet S, Kalager M. Mundal L, Skudal HK. Latvia. Diseases, health services and preventive medicine in Latvia. Student report, Institute of General Practice and Community Medicine, University of Oslo, Norway, 1996.
Antal EA, Lunde H, Tjora E, Voss C, lversen SM, Ødegård I. Diabetes, society and the concept of illness. A paper on diabetes care in Norway, Latvia, and the United States of America. Student report, Institute of General Practice and Community Medicine, University of Oslo, Norway, 1996.
Berntzen DTK, Engstrøm M, Opøien HK, Orrem J, Rustad DA, Spæren KH. Undseth RM, Yahyaei A. Tuberculosis, past or present? A comparative study of the prevention of tuberculosis in Norway, Latvia, and the USA. Student report, Institute of General Practice and Community Medicine, University of Oslo, Norway, 1997.
Alsaker C, Arnesen J, Enger H, Gretland T, Meinich P, Olsen KB, Ross lB, Vingen OS, Resistance. How to fight the microbes. A comparative study on the treatment of acute infections in Norway, Latvia, and the United States of America. Student report, Institute of General Practice and Community Medicine, University of Oslo, Norway, 1997.
Abeler K, Ausen K, Brandal P, Fossmark R, Gaupen Ø, Halsaa V, Hesstvedt L, Wiik T. Vaccination of children in Norway, Latvia and the United States. Student report, Institute of General Practice and Community Medicine, University of Oslo, Norway, 1998.
Aune E, Bakka N, Bliksrud YT, Garnes M, Skaar AC, Størset R, Thorstensen A, Qiao S. Asthma in Latvia, Norway, and the United States: a study of prevalence, incidence, and treatment. Student report, Institute of General Practice and Community Medicine. University of Oslo, Norway, 1998.
Askestad B. Bakken AM, Dalsveen H, Nes SB, Sletner L, Smestad C, Torgersen K, Vilming B. Arterial hypertension in Norway, USA and Latvia. Student report, Institute of General Practice and Community Medicine, University of Oslo, Norway, 1999.
Friis CM, Midtbu JE, Moen MC, Sæverud T, Taraldrud E, Tveito K, Tverå E, Ulimoen G. Årving I. Hormonc replacement therapy in menopausal women. Student report, Institute of General Practice and Community Medicine, University of Oslo, Norway, 1999.
Heier M, Kyamme E, Mjåset C, Røsten HE, Salkjelsvik M, Salomonsen V, Stuen W, Syversen IF, Tømte Ø, Øverland T. Dyspepsia. The present status. A study of definition, prevalence, risk factors, diagnostics and treatment in Latvia, Norway and the Unites States. Student report, Institute of General Practice and Community Medicine, University of Oslo, Norway, 2000.
Bergum HM, Iversbakken HJ, Nilsen EB, Kjøl CE, Mauritzen S, Kringstad El. Depression – as a primary health care problem in Latvia and Norway. Student report, Institute of General Practice and Community Medicine, University of Oslo, Norway, 2000.
Schjesvold F, Nguyen ATLT, Tran PBN, Veiby IM, Buchacz JL, Hoelsbrekken TE. Sexually transmitted diseases as a primary health Care problem in Latvia and Norway. Student report, Institute of General Practice and Community Medicine, University of Oslo, Norway, 2001.
General practicioner
Baznicas Street 19/23, Riga, LV-1010, Latvia
guki@latnet.lv
Department of general practice and community medicine,
University of Oslo
p.o. box 1130 Blindern
N-0318 Oslo, Norway
oivind.larsen@medisin.uio.no
Department of general practice and community medicine,
University of Oslo
p.o. box 1130 Blindern
N–0318 Oslo, Norway
e.o.rosvold@medisin.uio.no